
A 67-year-old patient was admitted to hospital for confusion and dyspnea. According to her family, she has changed her behaviour in the last three days, confusion. Her history: diabetes (insulin therapy), COPD grade IV, a history of pneumonia two months ago. No injury, dysuria or diarrhoea. She did not travel in the past three months. Her family is healthy.
Admission lab results: leucocytes 20600, neutrophiles 89 %, creatinine 120 umol/l, CK 1745 IU/l, CRP 278, procalcitonin 2.41 ng/ml, troponin T 69 ng/ml, pH 7.2, base excess -14.5, pCO2 33 mmHg, glycemia 25 mmol/l, glycosuria, ketonuria, lactate 0.8 mmol/l.
The physical examination findings: somnolence GCS 3-4-5(12), neurologically without lateralisation, no meningeal signs, anicteric, fever 39.0 °C, dry mucous membranes. Obesity. Regular sinus rhythm, 90 bpm, 120/70 mmHg without the necessity of a support, periphery shows sufficient blood supply. Auscultation reveals crackles bilaterally, without wet phenomena, tachypnea 30/min, SpO2 96% with the support of nasal oxygen cannula. The abdomen is soft, without pain, without resistance. Peristalsis is present. Neither oedema nor infection signs of lower limbs are present.
Chest X-ray did not reveal any apparent infiltration:

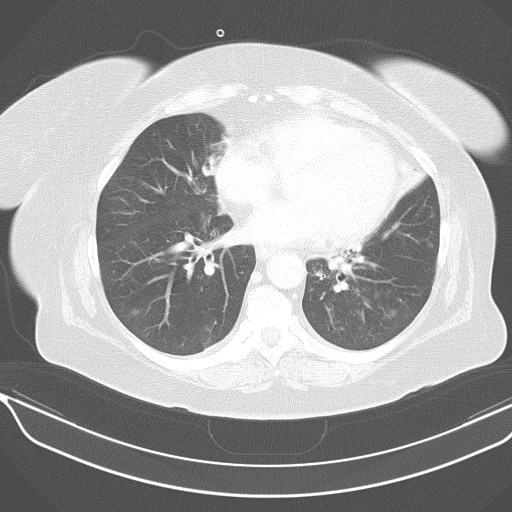
Chest X-ray revealed a tip extension of heart shadow in the direction of the thoracic wall. Chest CT performed two months ago showed a correlate to this finding. Thus, the finding can be considered stationary; this is not infiltration:
Diagnosis by the admission: bronchitis, decompensation of diabetes with ketoacidosis, dehydration and neuroinfection should be considered in the differential diagnosis.
Bed-side ultrasonography, looking for focus: