
Following cases show two patients who were admitted to the hospital for erysipelas. Both patients had to be admitted at ICU due to consciousness disorder (resulting probably either from septic encephalopathy or from toxaemia) requiring intubation and mechanical ventilation.
Patient number 1
Mild disease course, local symptoms were already in regression, blood cultures were positive for group-G beta-haemolytic Streptococcus.

Ultrasonography:

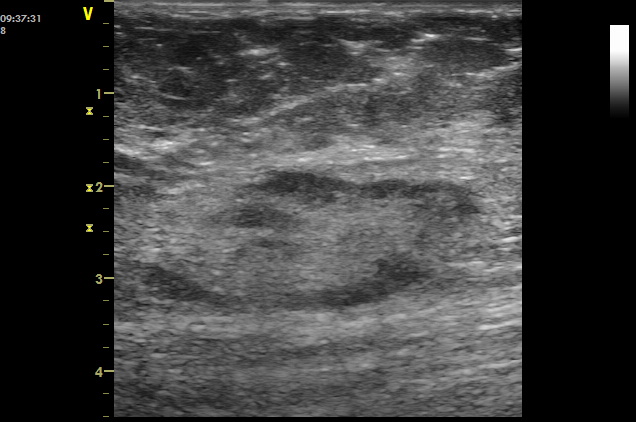
Sagittal scanning plane ventrally at the upper third of right calf (above the redness)
Skin and subcutaneous tissue show a width of 2.30 cm. There is the deep fascia visible below them. Thickening of subcutaneous tissue. Hypoechogenicity of adipose tissue with hyperechoic septa is preserved.
Transverse scanning plane ventrally at the upper third of left calf (above the redness), moving the probe craniocaudally and back
Skin and subcutaneous tissue show a width of less than 2 cm. Below them, there is the deep fascia visible as well as muscles with longitudinal septa (which are visualised at transverse scanning plane in this case). Thickening of subcutaneous tissue, hypoechogenicity of adipose tissue with hyperechoic septa is preserved.
Healthy right calf for comparison:

Sagittal scanning plane ventrally at the middle third of the right calf
Skin and subcutaneous tissue show a width of 0.75 – 1.0 cm. Below them, there is the deep fascia visible as well as muscles with longitudinal septa.
Examination of the left calf at the level of redness followed:
Sagittal scanning plane ventrally at the middle third of left calf (at the level of redness)
Skin and subcutaneous tissue show a width of 1.5 cm. Below them, there is the deep fascia visible as well as muscles with longitudinal septa. Thickening of both skin and subcutaneous tissue, hyperechoic adipose tissue with hypoechoic regions which correspond to fluid in septa.

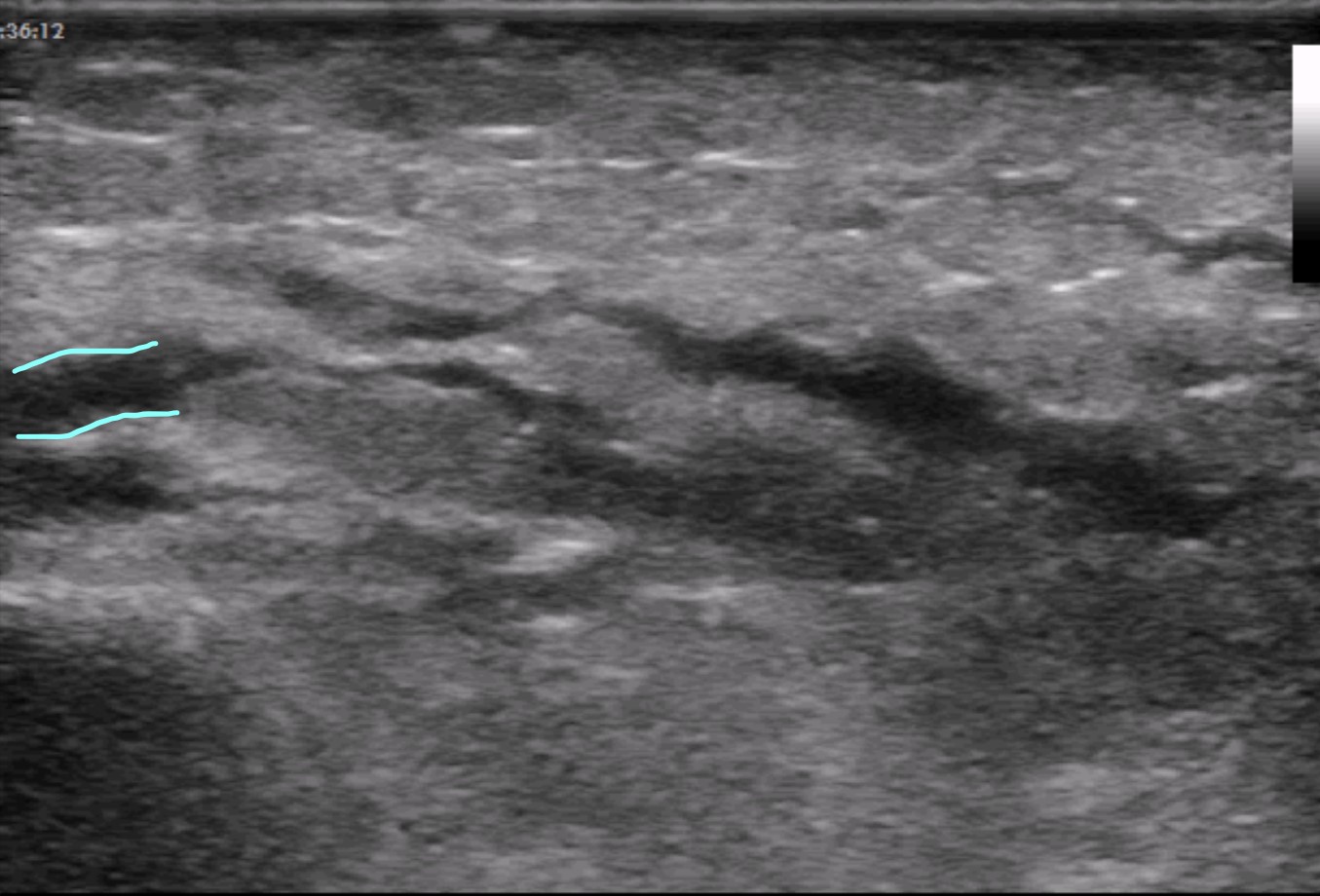
Transverse scanning plane ventrally at the middle third of left calf (at the level of redness), moving the probe craniocaudally
Skin (above yellow line) and subcutaneous tissue show width of 1 – 2 cm. Below them, there is the deep fascia visible (red colour) as well as muscles with longitudinal septa (which are visualised at transverse scanning plane in this case). Thickening of both skin and subcutaneous tissue, hyperechoic adipose tissue with hypoechoic regions which mount on the deep fascia at some places (blue colour).
Transverse scanning plane ventrally at the middle third of left calf (at the level of redness), moving the probe craniocaudally
Skin (above yellow line) and subcutaneous tissue show width of 1 – 2 cm. Below them, there is the deep fascia visible as well as muscles with longitudinal septa (which are visualised at transverse scanning plane in this case). Thickening of both skin and subcutaneous tissue, hyperechoic adipose tissue with hypoechoic regions. Fascia itself is surrounded by fluid only in the small part of the scan (blue colour).

Transverse scanning plane at the left inguinal region
Reactive lymph node at the transverse axis, hyperechoic hilum leaving lymph node ventrally is visible.

Transverse scanning plane at the left inguinal region, power Doppler
Reactive lymph node at the transverse axis, hyperechoic hilum leaving lymph node ventrally is visible.
Transverse scanning plane at the left inguinal region, power Doppler
Reactive lymph node at the transverse axis, hyperechoic hilum leaving lymph node ventrally is visible.
Sagittal scanning plane at the left inguinal region
Reactive lymph node at the longitudinal axis, hyperechoic hilum leaving lymph node ventrocranially is visible.

Sagittal scanning plane at the left inguinal region, power Doppler
Reactive lymph node at the longitudinal axis, hyperechoic hilum leaving lymph node ventrocranially is also visible. Central vessel branches to the periphery of the node.
Ultrasonography of the right wrist was also performed because the patient complained of pain in this region:
Sagittal scanning plane across the dorsum of right wrist, PDI
Thickening of the synovial layer without signs of activity. Compression does not push hypoechogenic structure away, pointing out to hypertrophy of synovial layer (and not to an effusion) in the wrist joint. Power Doppler shows just motion artefacts and nutrient vessel. Superficially, there are tendons of extensor muscles without signs of tenosynovitis. Bones do not show signs of fracture, erosion or osteophytes.
Patient´s condition did not require any surgical intervention.
The case continues here.